Contact: a.tuckova@paliativnicentrum.cz
Background
International evidence demonstrates that gender significantly influences access to and quality of healthcare, shaping needs, experiences, and expectations regarding end-of-life care. In the Czech Republic, women live approximately six years longer than men, and strong cultural norms persist regarding gendered caregiving roles. This longevity gap creates a specific dynamic: women often outlive their spouses, leaving them without a partner caregiver in their final years. Consequently, they rely more heavily on adult children, who frequently reside separately, increasing the likelihood that elderly women will transition to institutional inpatient hospice care rather than remaining in home-based settings.
Aims
This study examines whether gender affects access to hospice care in the Czech Republic, with particular attention to differences in patient demographics, caregiver composition, and care experiences across hospice types (home-based versus inpatient).
Methods
Data were collected between January 2023 and December 2024 in 17 hospices (14 home-based and 3 inpatient) using three complementary measurement tools:
- Cumulative Structural Data: Organizations varied in size, from large facilities serving ~40 patients monthly to smaller ones treating ~50 patients annually, ensuring representative coverage of Czech hospice services.
- Patient Cards: Individual records captured only patients who died in hospice care, documenting admission dates, death dates, age, diagnosis, condition upon admission, and care provided. The dataset comprised 5,789 individual patient records.
- Bereaved Feedback: Questionnaires were distributed 4–6 months after death to primary caregivers via mail and online platforms. A total of 2,700 questionnaires were analyzed, covering care aspects including symptom management, communication, psycho-spiritual support, and accessibility.
Quantitative data were analyzed using chi-square tests and adjusted residuals (p < 0.05) to identify statistically significant differences in gender, age, and caregiver relationships. Open-ended responses underwent thematic analysis, revealing key topics such as care quality, staff approach, environment, communication, availability, and timing.
Results
Bereaved relatives rated hospice care highly (average 9.8/10), with satisfaction consistent across both inpatient and home-based settings. However, significant gender patterns emerged regarding patient distribution and caregiver roles, strongly influenced by the age differential between genders.
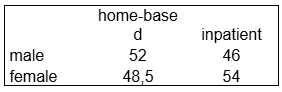
Gender Distribution by Hospice Type
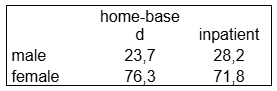
The overall gender ratio among patients according to Patient Cards was balanced, but significant differences existed between hospice types:
In the Bereaved Feedback sample (representing those whose relatives responded), the distribution was similar:
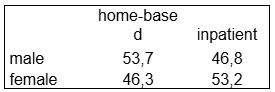
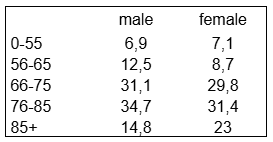
Key Gender Findings:
1. Age and Setting Correlation: Younger men (66–75 years) were more likely to receive home-based hospice care, often supported by spouses. In contrast, older women (76–85 years and 85+) predominated in inpatient settings. This aligns with the demographic reality that women live longer, often outliving their spouses, and thus rely on children who may not be able to provide 24/7 home care due to distance or other commitments.
2. Caregiver Composition: Caregivers were predominantly women (76% in home-based, 72% in inpatient hospices), typically middle-aged (46–55 years). While offspring (daughters) predominated in both settings, wives and partners were significantly more common as primary caregivers in home-based hospices.
3. Caregiver Burden: The most frequent difficulties included exhaustion, responsibilities for other family members, employment demands, and caregivers' own health problems. Despite the mental and physical demands, the perception of care 4–6 months post-death remained overwhelmingly positive.
Women's Voices
Bereaved caregivers shared powerful testimonies highlighting both gratitude for the care provided and the immense strain of the caregiver role:
These accounts underscore the dual reality: exceptional care quality alongside significant caregiver strain, primarily shouldered by women.
Discussion
Findings highlight gender as a key factor shaping access to hospice services, deeply intertwined with life expectancy and family structures. The data confirms that women's longer lifespan fundamentally alters their end-of-life care trajectory. Because women frequently outlive their spouses, they lack the primary partner caregiver that men typically have. Instead, they rely on adult children (predominantly daughters), who often live separately and face competing demands such as employment and their own families. This structural reality makes continuous home-based care more difficult to sustain for elderly women, leading to a higher proportion of women entering inpatient hospice facilities compared to men.
Conversely, men, who generally die at a younger age and are more likely to be married to a spouse of similar age, are more frequently cared for at home by their partners. This results in a distinct gendered pathway: men accessing care younger and often at home, while women access care later in life and more often in institutional settings.
While overall patient gender ratios are relatively balanced, meaningful disparities exist in:
- Age at access: Men tend to enter care younger, while women access inpatient care at advanced ages due to widowhood and lack of spousal support.
- Caregiver identity: Women overwhelmingly fill the caregiver role, with distinct patterns between spouses (home) and children (inpatient).
- Caregiver burden: The systemic reliance on female caregivers creates specific vulnerabilities regarding exhaustion and lack of respite.
Policies supporting shared caregiving responsibilities, workplace flexibility, and targeted respite care for adult children caring for aging parents could help reduce these disparities. Recognizing the link between gendered longevity and care settings is essential for designing a hospice system that is equitable and responsive to the specific needs of aging women.


